- Еуромедик, Булевар уметности 29, Београд
Ductectasias
Др Наташа Пујић Станисављев
Др Јелена Симовић
Одељење радиологије, Општа болница Сремска Митровица
What are ductectasias?
Ductectasias are enlargements of the milk ducts. Breasts consist of mammary glands that can produce milk. Milk is produced in parts of the gland called lobules.
From each of the lobules, milk flows into the final (terminal) milk duct (ductus) and together with it form the terminal ductal lobular unit (TDLU). Numerous TDLUs are connected to the system of milk ducts (subsegmental, segmental and main milk ducts) with which together they form a lobe. The human breast contains 15-18 lobes and each of them ends with the opening of the main milk duct at the nipple. The enlargement of any of the subsegmental, segmental and main milk ducts is called ductectasia.
How do ductectasis occur?
Enlargement of the milk ducts can be caused by the accumulation of fluid in them or by the accumulation of cells. The causes of fluid accumulation can be physiological (secretion of milk during breastfeeding) or pathological (when some benign or malignant process in the milk duct leads to the formation of fluid). When the canals expand due to the accumulation of cells in them, then it is most often malignant cells.
What are the physiological causes of fluid accumulation in the milk ducts?
During the breastfeeding period, the lobules and ducts of the mammary glands become very dilated because they are filled with milk.
Outside the period of milk secretion, ie. breastfeeding, throughout the woman’s fertile period, the lobules produce fluid. This cloudy fluid contains parts of cells (debris) and a high concentration of protein. Fluid secretion peaks during the secretory phase of the menstrual cycle, leading to premenstrual pain. This fluid is then resorbed in the canalicular system, rarely leading to the appearance of secretions on the nipple. Fluid resorption may not be complete and debris may accumulate within the canaliculi and cause them to dilate. The remaining alkaline, proteinaceous material that fills the ducts can calcify, which can be seen on mammogram images. This process is commonly called “secretory disease” or “plasma cell mastitis” and usually affects both breasts.
A number of women after entering menopause, in spite of lobular atrophy, retain enlarged milk ducts in the region immediately behind the nipple and areola. These fluid-filled ducts are surrounded by a larger amount of fibrous tissue, while in the rest of the breast, involution has occurred, replacing glandular tissue with fatty tissue. This type of structure of the breast is structure pattern III according to Tabar, it gives a specific image on a mammographic examination, and enlarged milk ducts are also observed during an ultrasound examination.
What are the benign causes of fluid accumulation in the milk ducts?
Hormonal changes can cause changes in the cells that line the mammary glands and lead to “apocrine cell metaplasia” – cells that produce a protein-rich fluid that is significantly different in composition from milk. Often this turbid fluid oozes from several openings on the nipples of both breasts. The color of the liquid can be gray, greenish, brown or yellow. If the liquid does not appear on the nipple, it remains in the milk ducts and leads to their expansion. This is how fibrocystic changes occur. Cysts are easily detected by ultrasound.
Another benign change that can be found within the dilated ducts is the papilloma, one of the few hyperplastic lesions of the breast that arise outside the terminal ductal lobular unit (TDLU) in canaliculi. The large amount of fluid associated with some papillomas dilates the ducts and their branches in the breast region between the papilloma and the nipple, often leading to the appearance of a serous (clear, yellowish) or bloody nipple discharge. If discharge is present, the best method for showing the location and number of papillomas is galactography. In other cases, the diagnostic procedures we apply are mammography, ultrasound and magnetic resonance imaging.
What are the malignant forms of ductal disease that lead to the accumulation of fluid or cells within the ducts and their enlargement?
A duct containing a papillary lesion may become cystically dilated due to fluid accumulation, and intracystic papillary proliferation may contain large areas of malignant cells grouped into papillary structures, and the lesion is then defined as encapsulated/intracystic papillary carcinoma. The diagnosis is made by pathohistological tissue examination.
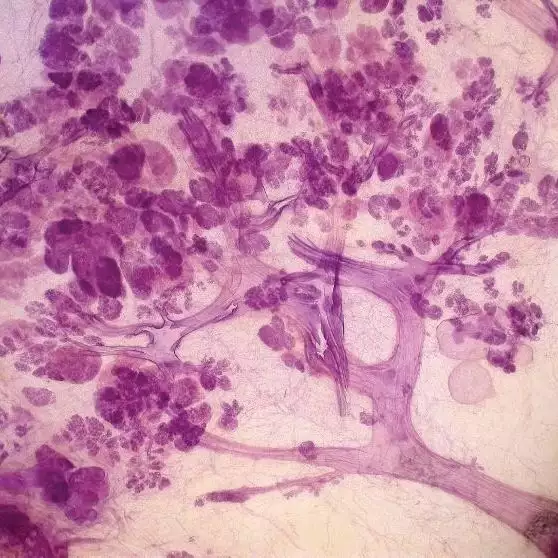
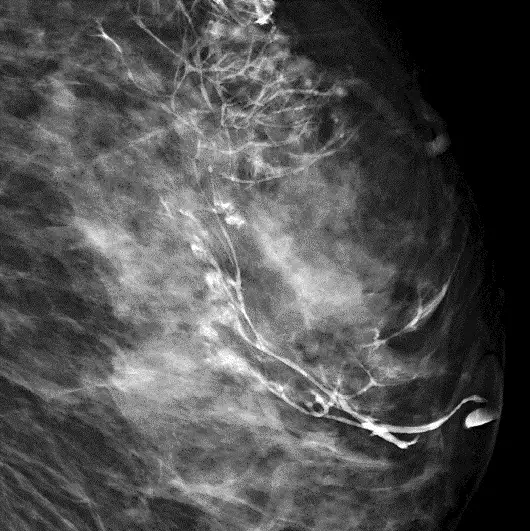
Ductectasias can also be seen due to the presence of a malignant process that develops from cells lining the main milk ducts (ductal adenocarcinoma of the breast – DAB according to the Tabar cancer classification). This type of cancer is characterized by the formation of new ducts, i.e. the process of neoductogenesis, where we see that the newly formed ducts have an irregular flow and branching pattern, are twisted and densely arranged next to each other, and that they do not have associated TDLU. It is a large neoplastic process that most often extends from the nipple to the chest wall, which leads to a large burden on the body with tumor cells. Unfortunately, this type of cancer behaves as an invasive cancer with a poor prognosis in about 30% of cases, and its name high-grade/poorly differentiated/Van Nuys group 3 type ductal carcinoma in situ – “DCIS” is still common. If malignant cells cover the inside of the ducts in the form of numerous layers of cells (solid type of growth) or in the form of papillary shoots (micropapillary type of growth), the ducts expand due to excessive accumulation of cells. If there is an insufficient supply of cells with nutrients from the blood, the process of necrosis (death) occurs in the parts of the tumor farthest from the wall (in the central part of the canal in the case of solid or at the top of the papillary shoot in the case of micropapillary growth) and the necrotic parts calcify. Calcifications can be seen on a mammogram of the breast, often as the only sign of the presence of cancer, which is already large in size. Micropapillary and cribriform (with the formation of spherical cavities) type of growth of tumor cells within the ducts can also lead to the accumulation of fluid secreted by these malignant cells. Fluid, serous or coagulated, may ooze from a canal on the nipple, and then the method of choice is galactography. If the liquid does not flow out, but accumulates in the milk ducts, it leads to their expansion (ductectasis). Non-calcified parts or the entire carcinoma with neoductogenesis can often be diagnosed by magnetic resonance imaging.
What are the methods of treating ductectasis?
Secretory mastitis and fibrocystic breast dysplasia are not conditions that require treatment. If cysts of large dimensions are formed in fibrocystic dysplasia, which lead to discomfort or pain for the patient, they can be emptied by needle puncture under ultrasound control.
Individual papillomas do not need to be surgically removed after proof of the presence of a benign papilloma by core biopsy. If there are a large number of lesions (multiple changes within the ducts that have a papillary appearance), we can prove the nature of one of them by biopsy, which does not exclude the presence of malignant cells in the other lesions, and surgical excision of the entire diseased segment of the breast is suggested after it has been marked preoperatively by a radiologist. When pathohistological analysis of the core-biopsy specimen shows malignant papilloma or intracystic carcinoma, wide surgical excision is recommended because of the high rate of associated carcinoma in situ (CIS) and subsequent recurrence of malignancy.
Carcinomas characterized by the occurrence of neoductogenesis require a radical approach in surgical treatment by the type of total mastectomy without sparing the skin and the nipple, because this process extends along the entire diseased lobe, from the main outlet milk duct whose opening is on the nipple to the chest wall.
Литература
1.Tot T., Tabár L., Dean PB. Practical Breast Pathology. 2nd Edition. Thieme Verlag, Stuttgart. 2014.
2.Tabár L., Tot T., Dean PB. Breast Cancer. Early Detection with Mammography. Casting-Type Calcifications: Sign of a Subtype with Deceptive Features. Thieme Verlag, Stuttgart. 2007.
3.Tabár L, Tot T, Dean PB. Breast cancer originating from the major ducts (DAB), Part 5 Fluid producing DAB subtypes with associated calcifications. 2015.
4.Tabár L, Tot T, Dean PB. Breast Cancer. The Art and Science of Early Detection with Mammography. Perception, Interpretation, Histopathologic Correlation. Thieme Verlag Stuttgart. 2004.
5.Tabár L., Tot T., Dean PB. Tarjan M. Prostate and Breast: Brother and Sister Organs. Hong Kong: C & C Offset. 2013.
6. Palazzo JP. Difficult Diagnoses in Breast Pathology Demos Medical, 1 edition. 2011.
7. Tibor T, Tabár L. Papillary lesions of the breast: histologic examination of contiguous tissue can predict the need for surgical excision. Poster exhibit at The 12th Annual Multidiscipline Symposium on Breast Disease. Febr 15-18, 2007.
8. Tabár L, Tot T, Dean PB. Ductal Adenocarcinoma of the Breast (DAB) Breast cancers originating from the major ducts, Part 2. Hong Kong: C & C Offset. 2014.
9. Tabár L, Tot T, Dean PB. Ductal Adenocarcinoma of the Breast (DAB) Breast cancers originating from the major ducts: Part 3. Hong Kong: C & C Offset. 2014.
10. Tabár L, Tot T, Dean PB. Ductal Adenocarcinoma of the Breast (DAB). Part I. Hong Kong: C & C Offset. 2014.
11. Tabár L, Tot T, Dean PB. Ductal Adenocarcinoma of the Breast (DAB) Breast cancers originating from the major ducts. Part 4. Hong Kong: C & C Offset. 2015.