- Еуромедик, Булевар уметности 29, Београд
Breast fibroadenoma
Прим др Милош Почековац
What is a fibroadenoma?
Fibroadenomas are benign tumors composed of the stroma of the breast lobule. Fibro-connective tissue, adenoma-glandular tissue.
About fibroadenoma
The World Health Organization defined a fibroadenoma as a “discrete benign tumor” showing the presence of connective tissue and epithelial proliferation. Fibroadenoma is the most common benign breast change that occurs in 25% of asymptomatic women. These are frequent changes in the breast from early reproductive life. It is caused by an imbalance of hormones. Fibroadenomas are benign tumors composed of the stroma of the breast lobules. This is the reason why fibroadenomas are most common between the ages of 15 and 25, when lobular development is most active.
They are usually single, but sometimes they can be multiple. They are most often present in the upper outer quadrant and are somewhat more common in the left breast. Fibroadenomas are more common in black people.
What is the cause of fibroadenoma?
The etiology of fibroadenomas is unknown, but the fact that lobular proliferation is a response to estrogen stimulation suggests that fibroadenomas arise as a result of estrogen action.
When does it appear?
Most often between the ages of 15 and 25, when reproductive life is most active.
Can lifestyle increase or decrease the risk of fibroadenoma?
The widespread use of contraceptive pills among young women makes it difficult to obtain accurate data on their role in pathogenesis. There is no evidence that the use of contraceptive pills increases the risk of developing fibroadenomas, but epidemiological data suggest that it may be associated with a reduced incidence. Most studies show that the risk of developing fibroadenomas is more than halved in those who take birth control pills, especially long-term users. Epidemiological studies indicate that progestogen is an element that has a protective role. An interesting study was published by Kani, which showed that women who take contraceptive pills and are under 45 years of age have a reduced incidence of fibroadenomas, and those over 45 have an increased incidence. Smoking appears to have a protective role with regard to fibroadenomas. In the study by Roan and Miller from Canada, there is a reduced risk of fibroadenoma in active smokers. Fibroadenomas are more common in women in higher socio-economic classes and in black women. They found that consumption of high amounts of vitamin C may be associated with a reduced risk of fibroadenomas, as well as body mass index and more pregnancies. Previous benign lesions as well as people under 35 increase the risk. Epstein-Barr virus may play a causative role in the development of tumors in immunosuppressed patients.
What types of fibroadenomas are there?
Simple or simplex, complex, multiple or multiple, giant and juvenile (in adolescents).
Are they all harmless?
Complex fibroadenomas can increase the risk of breast cancer.
Can fibroadenoma develop into breast cancer?
Cancer is a rare occurrence in fibroadenoma.
One study (Hagensen) showed only two cases in a period of 45 years of follow-up, which were lobular carcinomas in situ.
Another study (Diaz et al) reported 105 cases of carcinomas that were from fibroadenomas. The average age of the patients was 44 years, and the clinical characteristics did not differ from other patients with simple fibroadenomas. In 95% of cases there was carcinoma in situ in the fibroadenoma itself. Lobular and ductal tumor types were evenly distributed. No axillary nodal metastases were found. The authors recommended sparing breast surgery for carcinoma in situ arising from a fibroadenoma.
Some studies have shown that the incidence of cancer within a fibroadenoma is from 0.002% to 0.0125%. About 50% of these tumors are lobular carcinoma in situ, 20% are invasive lobular carcinoma, 20% are ductal carcinoma in situ, and the remaining 10% are invasive ductal carcinoma. Clinical, ultrasound and mammographic findings are similar to benign fibroadenomas.
How are fibroadenomas treated?
Fibroadenomas can cause physical deformity due to their size, discomfort or emotional distress. The patient must be familiar with the possibilities of treatment, both surgical and conservative methods, as well as the percentage of breast cancer.
Cryoablation is a recently described method (still not practiced in Serbia) for the eradication of fibroadenomas, and after establishing the diagnosis by core biopsy. Freezing technology (extremely cold liquid nitrogen) is used. This is a minimally invasive procedure. A probe or needle is inserted into the fibroadenum under ultrasound control. Argon gas flows through the probe and at its tip, the temperature drops to -196 degrees creating an “ice ball” that surrounds the fibroadenoma. After thawing, the probe is removed, and the fibroadenoma shrinks or disappears over time. The advantages are a small incision (3 mm on the skin), quick recovery, lower risk of infection compared to standard surgical interventions, no stitches and no change in the shape of the breast. First, the diagnosis of fibroadenoma must be confirmed by core biopsy.
As the method is simple, it is impossible to be sure that the fibroadenoma has been completely removed and hematoma is inevitable after the intervention.
SURGICAL TREATMENT
Indications for surgical treatment include:
- enlargement of the lesion during regular ultrasound examinations
- fibroadenoma >2cm
- uncertain diagnosis
- the patient’s anxiety
The classic surgical treatment is to excise the fibroadenum in its entirety through a small incision. Some surgeons recommend local anesthesia if the fibroadenoma is close to the skin, but for deep localized lesions, general anesthesia is most appropriate, both for the surgeon and the patient. Hospitalization lasts several hours.
The type of surgical excision depends on the clinical and radiological picture. The excision should be tissue sparing to avoid loss of glandular tissue. The scar should be as little visible as possible, made according to the principle of plastic surgery, both in terms of position and suture.
A submammary approach is usually advised, but sometimes the lesion may be distant from the incision, thus prolonging the operative time. It is recommended to mark the tumor preoperatively, on the skin, in the lying position of the patient with previous clinical and ultrasound examinations. In this way, we reduce the possibility of “missing” lies from the breast.
The most common types of incision are:
- Periareolar
- Submammary or inframammary
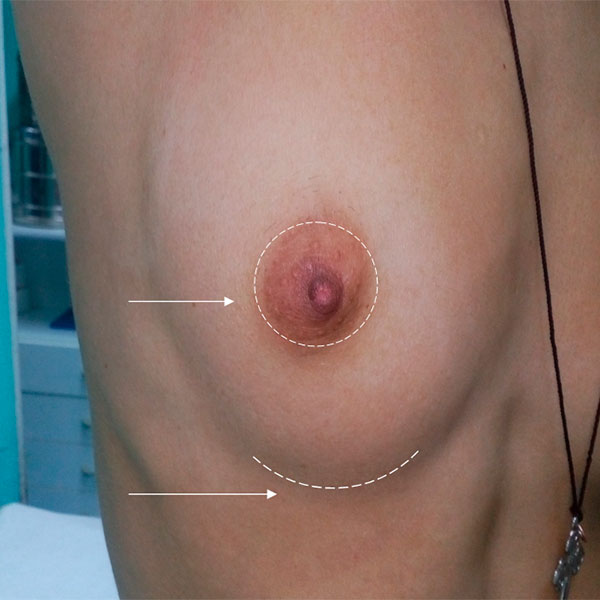
The first arrow shows the possibility of a periareolar incision depending on the localization of the change, and the second a submammary or inframammary incision.
A submammary or inframammary incision is also advised in the case of multiple fibroadenomas. It leaves a small deformity of the breast and can be repeated if there is a recurrence. The incision should be placed slightly above the inframammary groove, and in this way we can explore the entire breast.

A submammary incision that leaves a barely visible scar
The periareolar incision also leaves a barely visible scar and allows access to any quadrant of the breast. In this way, multiple fibroadenomas can be removed, as in the case of a submammary incision.

In the case of the patient, a needle biopsy of the change was performed 7 times on two occasions on the left breast and an uncertain histopathological finding was obtained, and at the request of the patient, it was completely surgically excised. A periareolar incision was made and the postoperative barely visible scar indicated by the arrow.
Histopathology report- fibroadenoma

The patient, afraid that it was a suspicious change, demanded a complete surgical excision of the change, which was about 2 cm.

Patient 18 years old with a positive family history. Out of fear, she demanded that two changes (histopathological fibroadenomas) localized in the upper inner quadrant and in the lower outer quadrant, be excised completely.

The arrow indicates a barely visible scar